Are you someone who has been dealing with nagging discomfort deep within the groin, glutes, or even under the sit bones? It may be time to examine your pelvic floor!
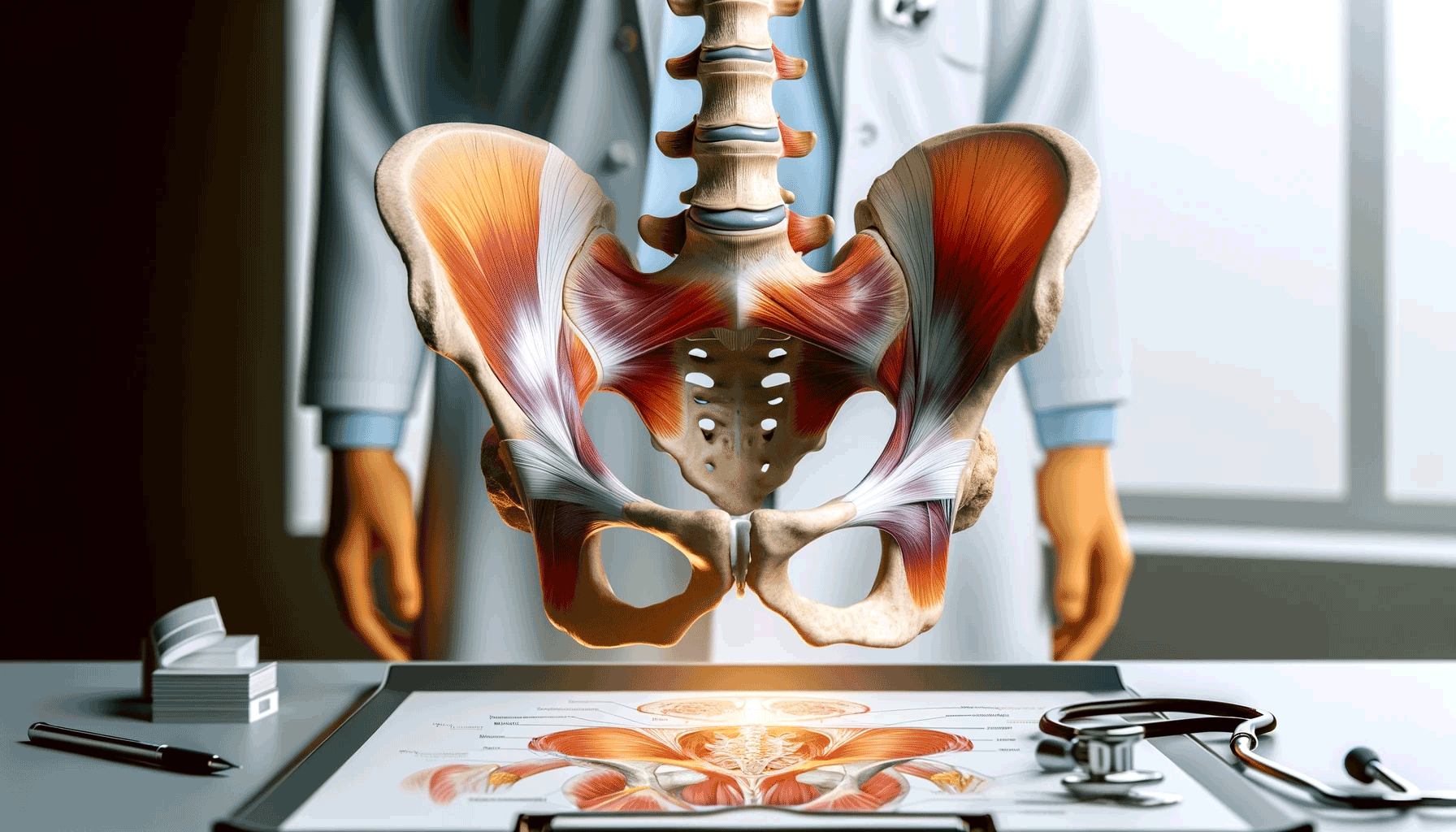
One of the key players during single leg stabilization and rotating the hip away from the body is the obturator internus. This muscle originates deep within the pelvis and exits to attach onto the top, outer portion on the back of the femur. This area also acts as a common insertion point for the majority of the hip's external rotators, with the piriformis and gluteus medius attaching just above.
Tendonitis and bursitis in this area are very common and are often caused by increased friction from a tendon that is consistently under tension and stress. The piriformis and gluteus medius are often blamed as they frequently demonstrate weakness and contribute to pelvic instability. Treatment is then aimed at reducing inflammation, increasing length, and improving strength of the muscles external to the pelvis. Only a fraction of the problem is addressed, and symptoms tend to persist if the muscle belly of the obturator internus remains shortened internally.
Obturator internus injuries are difficult to distinguish from strains in the adductor or hamstring as well, given the proximity of their tendons to the common insertion site. The mechanism of injury is often difficult to recognize as the obturator internus can be injured by a fall on the sit bones or even with wide kicks away from the body. It takes time getting to the root of the problem, but once accurately diagnosed, patients respond well to targeted rehabilitation of the obturator internus.
The best way to get started is by visiting a pelvic floor physical therapist who will evaluate the mobility and strength of your muscles, and begin a treatment plan to improve their function and endurance.