So what does actual treatment for a concussion entail? In our last blog, we addressed the signs of symptoms of post-concussion syndrome, noting that an athlete may not return to play until the symptoms have cleared. More than 80% of concussions will heal within the first 3 weeks but for the 20% that do not – what interventions should one do?
Historically, post-concussion treatment is rest. This includes no electronic devices, social interaction, exercise and a dark room which all minimize stimulation. The reason behind this was that a concussion affects the autonomic nervous system (ANS) and its control of cerebral blood flow which is thought to exacerbate with uncontrolled activity. Research now suggests this may not be the case beyond the first few days and can have an adverse effect of depression, anxiety and physical deconditioning. Rest has been redefined to "Reasonable Rest" or "Sensible Rest." Too much activity is also detrimental. The goal is to find the balance which is why the Buffalo Concussion Treadmill Test was developed.
Dr. Leady et al developed a protocol to systematically evaluate a person's exercise tolerance who has sustained symptoms for more than 4-6 week (PCS -post concussion syndrome). This is the only known functional test to help increase exercise tolerance with PCS. The goal is to restore normal physiology with sub-threshold exercise. Some studies found that early strenuous exercise was detrimental. While moderate exercises levels, 14 to 21 days after a concussion, at 60% of max HR performed for 150 min/wk showed improved spatial memory, neuron repair and better cerebral blood flow.
The Buffalo Concussion Treadmill Test (BCTT) gives patients guidelines on when to stop exercising thus eventually being able to increase their overall endurance. The BCTT is based on the Balke Cardiac Treadmill Test which was developed for cardiac and orthopedic patients with monitoring of HR and BP. With the BCTT, all patients start at 3.6mph and 0% incline and increase their incline by 1% every minute starting at minute 2 until reaching their maximum incline. Exacerbation of symptoms or exhaustion warrant stopping the test. If exhaustion is not reached at the end of incline, the speed is increased at .4mph per minute until the limiting factors are present. If the symptoms are not aggregated by exercise or displayed after the test, then they conclude it may be due to a cervical injury or vestibular/ocular dysfunction and not a concussion.
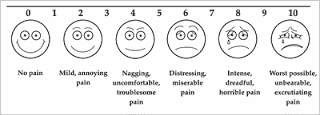
Visual Analog Scale
This test can be administered a few days a week if the patient is close to a full recovery. Otherwise, they suggest a graded exercises protocol. This includes aerobic exercise (bike, treadmill, elliptical) 20 min a day at a sub maximal threshold (80% of threshold HR achieved on BCCT) for 5-6 days a week. The first sign of symptoms requires they terminate any exercise. They can repeat the BCTT in 2 to 3 weeks and re-establish a new HR baseline and then return to the same process of graded exercise at 80% of new max HR. This is done until the symptoms cease to exist during exercise at 90% of age-predicted max HR for 20 minutes.
Although the BCTT protocol does not work for every concussed patient, it is a great tool to help in returning a child/adult to sports and activities of daily living. It gives concrete guidelines and boundaries to minimize symptoms in an area that has little to offer in the terms of protocols for concussed patients.
Reference
John J. Leddy, M. F. (2013). Use if Graded Exercise Testing in Concussion and Return-to-Activity Management. American College of Sports Medicine, 370-376.